


Shit doctors
There is no polite way to introduce the topic for this issue of The Autism Tribune.
Today’s exhibit from the autism archive captures chronic constipation in a very small child.

The image was taken by an x-ray machine at the Chelsea and Westminster Hospital in London on 14 March 2008. Our son was 4.5 years old. He had ingested laxatives and a small pot of radiopaque markers - which are small bits of plastic with a special coating to show up on the x-ray. The image told us what we already knew: his bowel had stopped working.
It’s hard to make out in the grainy image taken from the x-ray, but an image from a healthy bowel would have revealed a neat band of concentrated plastic bits moving together through the bowel. Our image shows the reverse; the plastic shards are distributed throughout the bowel, from top to bottom, left to right. The bits of plastic were floating around impacted faeces that was stuck to the walls of the bowel. The image captured the lack of bowel motility that would ordinarily allow a human being to expel solid waste. Without such motility, death would occur – and does occur - from lack of food, inadequate nutrition, bowel perforation and/or toxic shock.

The x-ray image captures the bowel problems that have plagued our son for years.
From the age of about 2, he often had what looked like diarrhoea which we later learned was the liquid passing alongside the faecal impaction. He filled countless nappies with brown liquid at the same time as having terrible constipation. He often barely ate. Nothing could go in as nothing could come out. His limbs were thin and his gut was distended - just as you would see in children suffering from famine in poorer parts of the world. He would shift his hip to one side and strain to produce tiny pellets of hard poo in his nappy. He would spend a lot of time rubbing his lower gut on the arms of chairs in the house. It looked like an urge for sexual relief but in hindsight we knew it to be a quest for the relief of what must have been terrible pain in his gut.
In those early days we knew nothing about the link to autism. All we knew was that our son was in terrible trouble. We spent a lot of time at the local GP surgery, asking for laxatives. We tried liquid paraffin (and remarkably this is still a recognised treatment), Senna and Movicol to try and help his bowel move. When nothing resolved the problem and at our request, we were referred to specialist paediatric gastroenterology services in early 2008.
After at least 2 years of chronic bowel problems, we were going to see the experts at the Chelsea and Westminster Hospital, and we went with great hope. The early x-ray showed the appalling state he was in. A blood test also showed a high level of IGE and a positive RAST test for milk (and we’d already taken that out of his diet because it caused chronic eczema and screaming at night). It also showed some slightly unusual biochemistry (low potassium, high urea, low transferrin saturation which relates to iron in his blood) but the letter to our GP described these as ‘normal’. The problem of chronic constipation was also treated as ‘normal’.
We were told that ‘idiopathic constipation’ is common in young children. The established protocol for treatment was to carry on with the laxatives and just add in some more.
Without improvement, we were advised that the likely option would be for the insertion of an Antegrade Continence Enema (ACE) ‘tap’. This involves surgery to insert a stoma in the wall of the bowel that can then be used to flush from the top down. It is a mechanical solution to a bowel that won’t work. Once installed, you sit on the loo and turn on the tap and this will empty your bowel as illustrated below.

‘Idiopathic constipation’ sounds rather benign but it just means the doctors have no idea what is causing the problem. Furthermore, it means they have no solution other than using laxatives or surgery, and no interest in getting to the root of the problem.
Using the labels ‘faecal impaction’, ‘mega-rectum’, ‘soft-stool constipation’, ‘pan-colonic inertia’ or ‘ileal-lymphoid-nodular hyperplasia’ better reflects the reality of living with a bowel that won’t work. The latter is the condition that Andrew Wakefield and colleagues saw and named in children with autism and GI problems when they started to look at what had gone wrong.
They used fancy medical language to capture what I have come to think of as ‘eczema of the bowel.’
Anyone with atopic eczema will know what I mean. When your eczema is triggered, the skin develops small fluid-filled blisters that are incredibly itchy. When you scratch, they can get infected and over time, the damage leads to crusts and cracks in the skin. For many people, it is a lifelong condition affecting the epithelial layer of the skin.
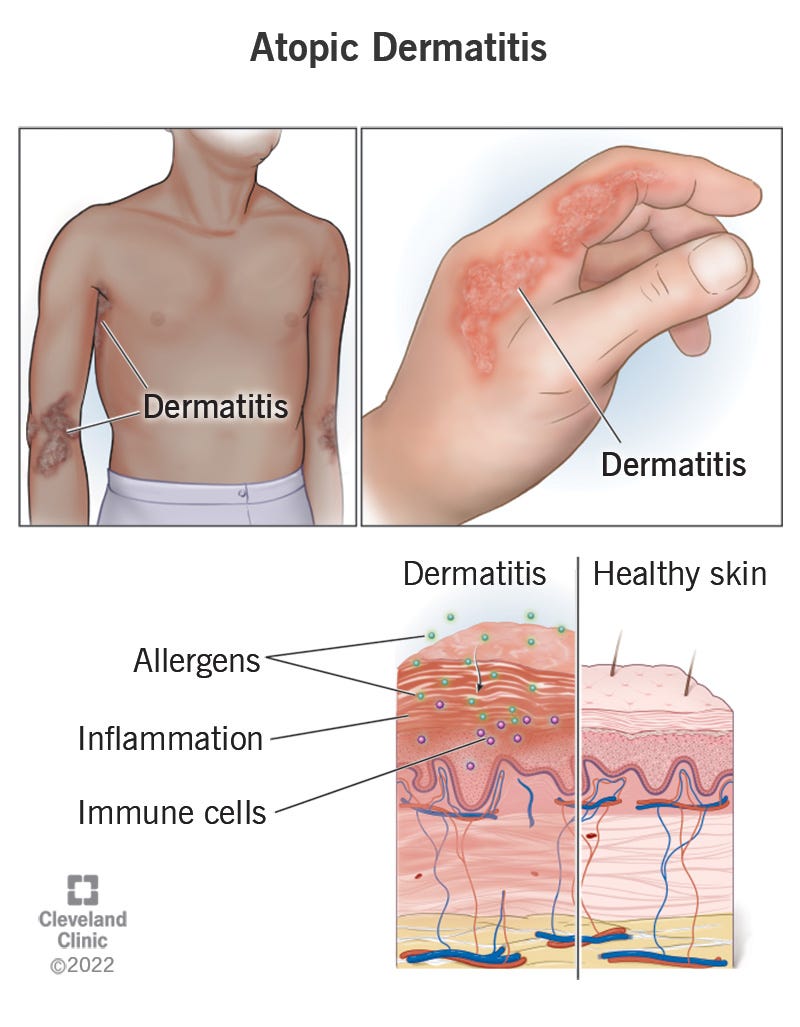
The GI tract similarly depends on the condition of the epithelial layer that stretches from the nose and mouth to the anus. It is critical to human immunity and once triggered, demonstrates a similar inflammatory response.
This is what explains the elevated numbers of swollen nodules of lymphoid tissue in the bowel of children with autism. It is like an eczema in the bowel and will impact on the organisms living in the bowel (the microbiome) as well as the physiology and the biochemistry of the GI tract, with implications for the rest of the body and most obviously, the brain.
There is nothing normal about a bowel that doesn’t work. It is a red flag that something is seriously wrong.
Young children who are suffering the twin and related regressions of bowel function and mental capacity can’t tell us how they feel. They need us to make sense of what is happening to them. They should be our top priority but most are left neglected, unassessed and untreated.
This, of course, is what Andrew Wakefield and colleagues were trying to address before they were stopped more than a decade ago. Their research identified immune inflammation in the bowel and they were exploring the possibility that low-level persistent viral infection - as already understood in relation to measles - might be causing the problem.
In contrast, the doctors and managers we encountered at the Chelsea and Westminster Hospital were hiding behind poorly written protocols that allowed them to do nothing. They had queues of children coming to see them and they did nothing more than prescribe laxatives and advocate surgery. I still find this hard to believe.
Rather than wait for nothing or worse, we ended up administering nightly enemas to clear our son’s bowel for ourselves. We later found a private hospital with doctors who were willing to help and we paid for tests to look at his GI function, associated biochemistry and the ecosystem of micro-organisms found in his bowel. We found that low-dose neomycin (a broad-spectrum antibiotic) allowed him to sit on the loo and do a marvellous poo. We found a complete absence of lactobacillus in his bowel despite months of supplementation, as well as patterns of dysbiosis that remain a problem today. We also found that he had very high levels of anti-bodies to Cytomegalovirus (CMV), Herpes Virus type 6 (HHV-6), Measles and Varicella zoster (chicken pox) that were never explained. With limited resources, we tried to understand what was happening and what we could do – a mission we continue almost 20 years later and likely for life!
After more than two years of repeat appointments for nothing, we wrote to the medical team and Heather Lawrence (now OBE), then Chief Executive Officer at the Chelsea and Westminster Hospital, to share our experiences of alternative treatments and raise our concerns.
The letter dated 16 May 2010 included the following:
“We find it increasingly difficult to understand how you and the NHS were unable to treat [our son] and showed so little interest in his condition and yet another doctor was able to transform his treatment in just one consultation. When we came to see you, [our son] had extreme abdominal bloating, he was in severe pain with the constipation, he had a very limited appetite and was very small for his age. He cried a lot of the time and was clearly not well. To us, bowel failure is a very serious condition and yet it appears to be viewed as a rather minor condition. With hindsight, we feel it was completely inadequate to hand us a bottle of Senna and some sachets of Movicol and tell us to come back in a number of months.
We hope our letter will encourage you to try additional treatments using more testing and antibiotics for children like ours. Our son’s case clearly indicates scope for dramatically improving the well-being of children with severe bowel problems.”
Three months later and following an ‘internal case review’ involving the consultant paediatric gastroenterologist, a consultant community paediatrician with expertise in neuro-disability and the Divisional Medical Director, we were given an official response.
The letter, dated 26th August 2010, said that the team had followed ‘the clinical algorithm for chronic constipation’ and that this held for those with Autistic Spectrum Disorder (ASD) as well. We were told that ‘constipation is a common problem in children with autism’ (who knew!) and that the team have experience of ‘effective management’ of these cases (which means laxatives and surgery).
The review panel were ‘delighted’ that we had found solutions via a private provider but “part of our duty as an NHS organisation is to offer evidenced based care, approved and mandated by the National Institute for Clinical Excellence (NICE) and expert opinion.”
We were told that our treatment was “outside of nationally sanctioned guidance [and] as such, until it is shown to be safe and efficacious when properly investigated in clinical trials, this treatment remains unproven for general NHS practice.”
They appreciated that our experience had been ‘frustrating’ and thanked us ‘for taking the time to make us aware of the success of the new treatment undertaken’ (you can bet they were thankful!)
What can you say?
This unofficial ‘treatment’ of ours involved using diet, probiotics, enemas and antibiotics to treat chronic constipation. It is hardly off-piste. It is just common sense.
Hiding behind the ‘protocol’ of the ‘algorithm’ means leaving children in pain and likely exacerbating their ‘autism’ (which is obviously related to the neuro-immuno-inflammation found in the gut and amplified in the neurological signalling that reaches the brain).
It is hard to understand why doctors complete up to 7 years of medical training to end up following a protocol that leaves children unwell while actively preventing them from finding out what has gone wrong. The politics of this stink to high heaven and what’s more, nothing has changed to this day.
The official guidelines developed by the National Institute for Care and Clinical Excellence (NICE) in relation to treating constipation in children and young people (CG99), last updated in July 2017, no longer recommends the transit test with which I opened this post. Everything is about maintenance with drinking water, fibre, exercise, laxatives and if all else fails, the ACE tap as was on the table for us.
Furthermore, and as mentioned on the Autism Tribune before, the NICE guidelines for ASD in under 19s (CG128), advise (in section 17.1) against medical investigations as part of the assessment. There is no recognition of comorbid bowel problems nor any attempt to investigate, understand or treat the condition. Nothing has changed in almost two decades except that rates of autism continue to rise, and it is no longer called a disorder but rather a ‘gift’.

Guardian 18 Feb 2025
The numbers of children admitted to hospital for constipation have also risen dramatically during this time – up 60% in the decade to 2024 (with 44,000 children being treated in 2024 alone). Many of them will have related immuno-neurological inflammation in the gut and the brain that is completely ignored. Indeed, the media coverage accompanying the data put the problems down to ‘emotion and diet’, with the implication being bad parenting and smart phones were to blame, rather than anything like allergy and inflammation in the wall of the bowel.
I suspect that many of the children reported to be starting school unable to use a potty are also suffering from unrecognised constipation and neurological problems. The parents are blamed.
The doctors are following protocols which mean they leave their brains at the door of the hospital. The children are left unwell and worse. The families carry the pain and the tax-payers pick up the bill.
The health and happiness of our children should be our top priority in life. We have forgotten one of the most basic lessons of the New Testament; “the kingdom of heaven belongs to the little children” (Matthew 19:14). The experiences of children with disabilities left with chronic constipation is a sign we have forgotten it all. The Autism Tribune is devoted to reminding everyone before it’s too late.
This is just shocking. Every post you write leaves me speechless and in awe of the lengths you went to find solutions. I’m distraught that you and your son were so desperately failed by ‘the system’. All you say makes such sense and explains what’s going on with a couple of children in my life and many others not so closely connected. It’s hard. 😢
Thanks for sharing your story,, Jane. This sadly is the state of health-"care" in the West today. We have the same issues here in Amerika, Inc., but no OBEs to hand out to compliant healthcare workers - just stock options and board seats in the managing corporations, occasional bonuses, and academic or political appointments, for the most corrupt. Thank your for your voice and for being a warrior mom.