


I forgot the psychiatrist!
Autism and the medical division of labour
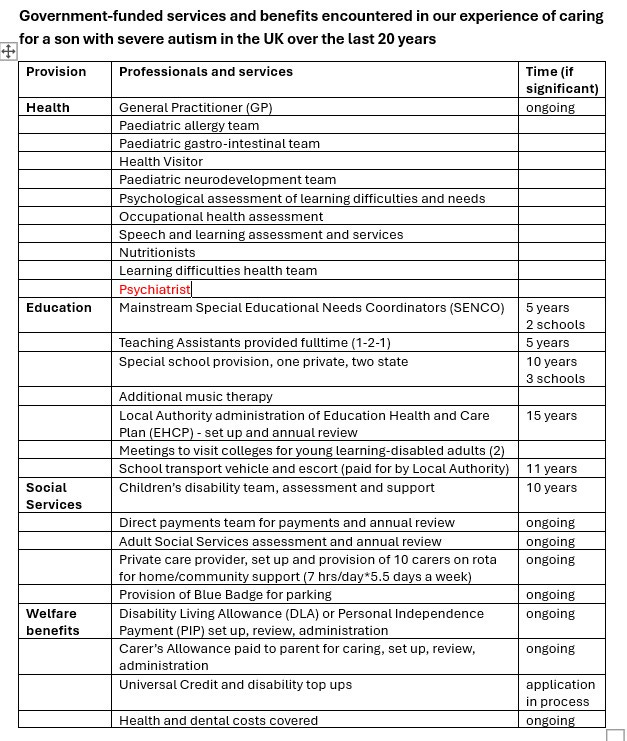
In my last post I focused on the cost of autism and the associated Autistic Service Delivery (ASD) industry that has grown up alongside the exponential increase in people affected. I provided a table listing all the state-funded services and benefits we have encountered in caring for our son with severe autism over the past 20 years, divided into sections capturing health, education, social services and welfare benefits.
Lying in bed the night after posting, I realised I had forgotten our encounter with a psychiatrist – and this needed to go in the section on health (now corrected in the new version of the table below). This brings the number of different services in the table to 27, adding to the taxpayers’ bill and reflecting the size of the ASD-state.
I likely blanked out the psychiatrist because we met him at a very difficult time. We were referred during the summer before last (August 2023), when our son stopped eating and drinking and we were at our wit’s end. Given his limited cognition, we knew the anorexia was not a conscious decision, but it felt as though he wanted to die. Already small and skinny, he lost a great deal of weight and was fading away.
In desperation, we contacted the NHS learning difficulties team who dispatched a psychiatrist to make an assessment. He phoned and then visited, and we went over the same ground that we have covered with all the other medical specialists listed in the table above. He told us that while neurotypical people are generally assumed to have consciously decided to stop eating, he recognised that our son could not have made such a choice. It appeared that the area of our son’s brain that stimulates hunger and the drive to eat had shut down and none of us had a clue what to do.

Our own google searches identified parallels to the way that cattle will sometimes stop eating and drinking when they are deficient in certain minerals (calcium, phosphorous, magnesium, potassium and zinc). Many farmers will have seen this as any animal brain can lose function in the area that controls appetite and the incentive to eat. We got a good vitamin and mineral supplement and after 10 days of starvation were able to begin a diet of stewed fruit that slowly allowed our son to start eating again. To his credit, the psychiatrist did not pretend to have any answers or give him drugs that could potentially make his health worse, but he also had no idea about the metabolic processes causing the eating disorder, nor indeed, the connection to autism.
Revisiting this encounter has got me thinking about where autism sits in the medical division of labour. Over our time, we have seen the psychiatrist and several psychologists. These specialisms focus on behavioural problems and mental distress, but their focus is on thoughts, feelings and actions, and how to ameliorate symptoms with drugs. They don’t attend to the underlying causes of these conditions.
In contrast, the related specialism of neurology focuses on disorders of the brain and central nervous system, and its practitioners are more open to exploring the causes of the conditions they treat – not least because they are associated with a very obvious regression during the onset of symptoms. In these cases, you cannot deny that something has caused a catastrophic decline in a person’s health and well-being. Well-known conditions in this camp are Multiple Sclerosis, Parkinson’s, Alzheimer’s and Motor Neurone disease.
Given that our son’s regressive autism was a manifestation of some sort of metabolic disorder, with parallels to conditions such as Alzheimer's and Parkinson’s, with a similar deterioration in communication, cognition, memory, language, control over physical movements and coordination, you might expect him to be overseen by people working in the specialism of neurology. If there has been a decline of this order, something must have caused it to happen.
Since it first became fully recognised in the medical encyclopaedia, after the Second World War, autism has been overseen by the disciplines of psychiatry and psychology. The early researchers such as Leo Kanner, Michael Rutter and Lorna Wing belonged to the discipline of psychiatry. They carefully documented the unusual behaviours associated with the condition and over time, these were distilled to differentiate autism from other behavioural and mental disorders. The current version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) identifies autism with deficits in (1) communication; (2) social interaction; and (3) restrictive and repetitive behaviour, interests and activities. The manual argues that these characteristics should be present from early in life and cause significant impairment if you are to confirm the patient as having as Autistic Spectrum Disorder (ASD).
Witnessing our son’s dramatic regression into autism suggests that these behaviours are the outward manifestation of metabolic dysfunction that began during the second year of his life. He lost skills he’d already acquired and developed a range of disturbing behaviours and problems (in sleep, toileting, language, communication, empathy and self-control). Furthermore, the extent to which his symptoms change over time – sometimes very dramatically - depending on diet and environment, including his exposure to sunshine and the cycles of the moon (as outlined in the second post for The Autism Tribune), suggest that his biochemistry is not fixed and it underpins the way he behaves.
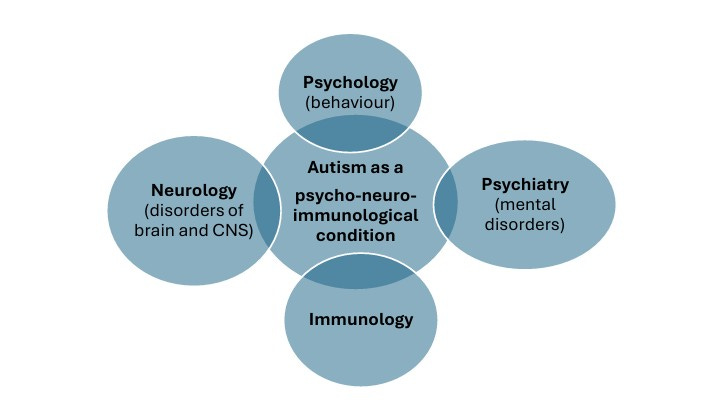
The emerging field of psycho-neuro-immunology might better capture the way that autism manifests as a set of behaviours that reflect underlying changes in biochemistry, neurological development and function. Understanding severe autism as a pathology with a biochemical explanation would help us unpack what is going wrong and identify ways to reduce and even reverse the dysfunction.
If your elderly relative started to lose cognition and previously acquired skills or started shaking uncontrollably, you would send them to a medical expert (likely a neurologist) to diagnose the condition and identify potential treatments. When your infant does the same – and for us the regression happened between the ages of 18 months and 4 years old – you do not expect to be told that this is just an issue of disordered behaviour without some explanation as to the underlying causes involved. Some of the most egregious symptoms of severe autism such as head-banging, aggression towards care-givers, screaming and crying, could be alleviated if they were understood to require the expertise of a combined perspective including psychiatry (focused on the manifest symptoms), neurology (exploring changes in the central nervous system including the brain) and immunology (looking at the biochemical signalling between body and brain that is likely at the root of the problem).
However, at the moment, the doctors assessing children with autism are under strict guidelines laid down by a government agency - the National Institute for Health and Care Excellence (NICE) – that direct them NOT to do any follow up investigations as part of the process. The panel overseeing these guidelines (officially published as CG128) suggest that doctors diagnose using the standard criteria in DSM-5 (communication, social interaction and repetitive behaviour) and do no more. They acknowledge the prevalence of what they call ‘co-existing’ problems in relation to anxiety, learning difficulties, epilepsy, feeding and sleep problems, as well as symptoms known to be associated with genetic disorders (such as Fragile X), but advise that these are considered additional to rather than constitutive of autism. Indeed, the guidelines go on to say (in paragraph 1.7): “Do not routinely perform any medical investigations as part of an autism diagnostic assessment” with exceptions only for suspected genetic disorders and epilepsy caused by encephalitis.

Being a parent of a child with severe autism I KNOW that the immune and bowel problems, the sleep disruption, the head-banging and learning difficulties (among many other things) are manifestations of an underlying metabolic disturbance. I have never understood how the doctors don’t want to acknowledge this and find out what is going wrong. Why spend years in medical training if you end up following the not-NICE guidelines that suggest you look at a set of symptoms, fill in the paperwork and say no more. Surely they know more than they are prepared to admit in public, and if that’s the case, we know that solving the puzzle of autism is more about politics than medicine. We need a political movement to change the way doctors and those who regulate them understand the condition. We owe it to the next generation to rethink autism, its causes and how to stop its devastating effects.